


Sommaire
- Point de vue de la direction de l’inspection (DI) de l’ANSM sur le document ICH Q12
- ICH Q12 : les fondamentaux. Retours des travaux du GIC A3P ICH Q12
- First steps towards ICH Q12: Leveraging process understanding & development data to define process Established Conditions
- ICHQ12 Implementation from an Industry Perspective with a Focus on Established Conditions
- ICH Q12 compliance and Unified Quality and Regulatory Information Management
- Burkholderia cepacia a encore frappé
- Nouveau guideline Stérilisation de l’EMA
- How to store highly sensitive drugs? The benefit of functional coatings
First steps towards ICH Q12: Leveraging process understanding & development data to define process Established Conditions
ICH Q12 is an opportunity for optimizing the regulatory management of the life cycle of pharmaceutical products, but it raises a lot of outstanding questions when preparing CMC dossiers. There is no detailed guidance on how Established Conditions should be justified and the boundaries between ECs/non-ECs and between ECs reporting categories are not well defined. Companies therefore need to establish their own methodology and dossier structure.

1. Introduction
ICH Q12 is the next important step on the way to the new pharmaceutical quality paradigm started with ICH Q8. Whereas previous ICH guidelines of this series mainly addressed issues dealt with by development and production teams, ICH Q12 will also require deep involvement of the regulatory teams preparing CMC dossiers for submission.
From a regulatory perspective, it has to be noted that ICH guidelines are not intended for veterinary medicines, for which specific VICH guidelines are issued. Nonetheless, this series of ICH guidelines, setting the general principles of quality management, has no reason to restrict to human medicines. Additionally, reference to ICH guidelines Q8-Q9-Q10 are encouraged for veterinary products even if not mandatory.
Apart from regulatory considerations, voluntary adoption of such approaches for veterinary CMC dossiers (Chemistry, Manufacturing, and Controls) can have an added value for more efficient and transparent communication with Agencies, as well as for easier life cycle dossiers maintenance and knowledge management within the company.
Considering this regulatory environment, but also the focus of the company on continuous improvement and innovation, our current initiatives for enhanced CMC dossiers understandably led us to try to introduce in dossiers some new concepts drawn on ICH Q12 approach. The first step taken aimed at having Established Conditions declared in CMC dossiers and assigning regulatory reporting categories.
Being a shift of paradigm, this initiated a deep revision of the structure of our regulatory dossiers. This was a gradual evolution over the last years, with a stepwise change in our methodology and dossier templates, nourished by gained experience and the variety of case studies.
This journey is shortly presented here from a CMC writer perspective, with questions raised, chosen options and the first feedbacks from Authorities.
2. Background and scope of application of the concept of ECs
Veterinary regulation is rapidly catching up the concepts already applied to human products. In the past years, greater emphasis was put in new or updated guidelines on risk-based approaches to pharmaceutical development and quality management, with clear encouragement to adopt the principles outlined in ICH guidelines Q8/Q9/Q10.
Moreover, at least for dossiers submitted in Europe, US or Canada, the dossier is reviewed according to the same general principles as for human products.
These were the first reasons for revising our CMC dossiers. The objectives defined were to secure regulatory review cycles and establish a science-based reference to efficiently rely on for products regulatory life cycle.
Even if ICH Q12 does not limit its application to the manufacturing process, our choice was to first apply the concept of ECs to manufacturing processes, for which post-approval scale-up, optimization or transfer can be foreseen. This choice also resulted from an increasing demand from Authorities for details in the description of manufacturing processes.
3. What current regulatory texts say about the level of process details to be included in CMC dossiers and management of process changes
The European guideline on product manufacture (CHMP guideline EMA/CHMP/QWP/245074/2015 for human medicines(1), and the equivalent CVMP version still in draft for veterinary medicines(3)) clearly indicates that “Consideration should be given … to what extent the assurance of quality of the finished product is founded on the manufacturing process itself…/… there is a need to describe the manufacturing process in relevant detail since consistent quality of a product cannot be safeguarded by end product testing alone”. It is also interesting to note that during the consultation phase, following the concern raised by the industry on the increased level of detail requested (as compared to previous guidance), it was clearly answered(2) that “contrary to the observation stated in this comment, assessors throughout EU have observed a tendency for companies to provide less and less information in the manufacturing section to the point that there is little or nothing to assess. Therefore it is not the intention to go back to the statements of the previous guideline, as these statements have been misused in the past by some companies”.
This increased focus of EU reviewers on process description in dossiers raises the following question: how can we provide sufficient details while not increasing the number of post-approval variations? In this context, it appeared to be the right time for introducing the concept of Established Conditions and counterbalance the higher level of detail requested by Authorities. At this point, the second question was: is it possible to already use the first part of ICH Q12 (identification and classification of ECs) in CMC regulatory dossiers?
Indeed, whereas process ECs are defined with respect to the process risk area specific to each drug (which may depend on raw materials properties, product pharmacokinetics profile and intended use of the drug product), such a customized approach may not always easy match current regional general requirements for the regulatory management of changes.
In Europe, the current legal basis for regulatory variations categorizes changes for non-sterilization process unit operations and non-biological products (section B.II.b.3 of current EU Regulation 1234/2008 on variations (4)), as either:
a) “Minor change in the manufacturing process” (Type IA variation),
b) “Substantial changes… that may have a significant impact on the quality, safety and efficacy” (Type II) or,
c) “Minor change in the manufacturing process of an aqueous oral suspension” (Type IB)
Condition 2 for categorizing a change as minor is defined as “Either the change relates to an immediate release solid oral dosage form / oral solution…./… or the change relates to process parameter(s) that, in the context of a previous assessment, have been considered to have no impact on the quality of the finished product (regardless of the type of product and/or dosage form)”. This last condition opens the door to the concept of ECs in dossiers if adequately supported by a risk assessment at the time of initial submission.
This is also in line with the revised EU guideline on product manufacture (1) (3) saying that “A well described manufacturing process is essential to understand what is critical and what is supportive. Any information which is considered to be purely supportive should be justified and clearly identified”.
As for US FDA guidance dealing with drug product manufacture and life cycle management (5 to 9), CVM GFI #234 guideline “Question-Based review for the Chemistry, Manufacturing, and Controls technical section of animal drug applications” clearly includes QbD concepts setting the basis for process risk analysis, and a draft guideline is already available for human medicines on Established Conditions. Moreover, the initiative for the GMP of the 21th century launched in 2004 officially claims the will to place focus on CMC risk area and reduce regulatory paper work.
To be complete, we can add that the concept of PACMP (Post-Approval Change Management Protocol) is also partly covered by the current regulation on post-approval change management protocols in EU and US, but this was not in the scope of our pilot phase.
This analysis of regulatory texts illustrates how current regulatory provisions could already be used for declaring process ECs even if ICH Q12 was not yet in place.
4. A prerequisite: a sound scientific basis presented to support ECs definition
The objective being set, the next question was: ECs being specific to each drug product, what elements will support the risk-based justifications (considering quality guidelines and industry state of the art practice)?
For sake of clarity and also willing to provide a comprehensive product quality analysis, QbD concepts of QTPP, CQAs, CMAs, CPPs and Control Strategy appeared to us the best way to structure data, ensure that they are complete and highlight the specific risk area of each product.
This does not necessarily means changes to the development pathway of products, as can be first feared when thinking of QbD as set forth in some high level scientific publications. Neither does it mean having to systematically test lengthy and costly process design spaces during development. In our approach, introducing QbD in dossiers was indeed more about structuring prior knowledge and available development data in the dossier through a Quality by Design presentation.
The approach is in fact flexible regarding the set of development data (can be completed by prior knowledge and scientific arguments), the area covered (e.g. can be done only for some process unit operations) and the final claims (manufacturing operational design spaces being optional). This leeway allows for a pragmatic customization of the strategy to the stakes of each project, which should be ideally defined in the early phase of pharmaceutical development.
It should however be emphasized that introducing a QbD approach with ECs in a dossier may require presentation of a more significant set of development results (even if not all) as compared to descriptive dossiers, along with thorough data analysis and justifications. The challenge is here to review development studies in details, sort what is relevant to support identification and classification of ECs, but present it with both rigor and clarity. CMC writers should therefore be involved in the early phases of pharmaceutical development, and sufficient time should be planned for drafting the CMC dossier.
5. Pilot dossiers: the strategy
Even if our first submissions of ECs were not formalized as a pilot project, we will refer to it as a pilot phase. The dossiers selected were prepared for international registration covering both European and US FDA submissions. As previously indicated, the concept of ECs was proposed for the manufacturing process only, with a focus on some unit operations.
ICH Q12 approach is also flexible regarding its extent: the approach can be limited to the identification of ECs versus non-ECs, or be further extended by assigning reporting categories and even downgrading categories through post-approval change management protocols.
In our pilot phase, it wouldn’t be accurate to state that we established a strategy from the start, which should normally be the case to ensure that all supporting development are available. In fact, in this pilot phase, we analyzed available development data to best leverage them to the extent possible and deemed reasonable from a regulatory viewpoint. Some case studies are shortly presented in this article.
QbD concepts were used as the basis for presenting development studies in the dossier, which required alignment with development teams. The pharmaceutical development section was the first dossier section drafted and was prepared early on to capture key information, establish the logic and have it reviewed by development teams, which quickly raised the first documentation questions on how to present the elements of the QbD logic, in the absence of any regulatory guidance.
6. The need to establish new CMC dossier templates
In Europe, veterinary dossiers are generally submitted using the NTA format, in which pharmaceutical development is presented in part II.A. As for the CTD format, there is no detailed structure for the part dealing with process development.
For the dossier of new products to be submitted outside Europe, we chose to adopt the CTD format structure, as allowed for veterinary products in both Europe and US (with some minor format adjustments).
When it came to drafting the dossier sections to present the QbD logic, it appeared that it was not that obvious. Revised internal templates had to be built in order to structure the logic in the dossier in a clear way for reviewers, and in a consistent way for internal use within the company.
The main questions pertaining to documentation were:
• Where present the QTPP and the analysis of CQAs?
• Where and how present the process risk assessment supporting CMAs and CPPs?
• How present process development data?
• Where and how present the resulting routine Control Strategy?
• Where and how present process ECs?
• How link ECs risk classification with reporting categories (defined per region) and where should it be presented?
• Given the flexibility of the approach and the absence of any guidance, how can we make the approach taken for each dossier clear for reviewers (who will receive as many dossiers presentations as companies)?
All these questions had also to be addressed from a long-term perspective, ensuring that the chosen options would allow for easy post-approval data supplementation while keeping a clear consolidated dossier. Indeed, one major objective of enhanced dossiers is to make it a useful reference for production units and regulatory teams during the product life cycle. This appeared to be one more reason for not presenting dossiers as purely narrative pharmaceutical development, but have it organized according to a QbD logic.
The central role of the development section for initial submission but also product life cycle is illustrated in figure 1.
7. Structure of the CMC dossier
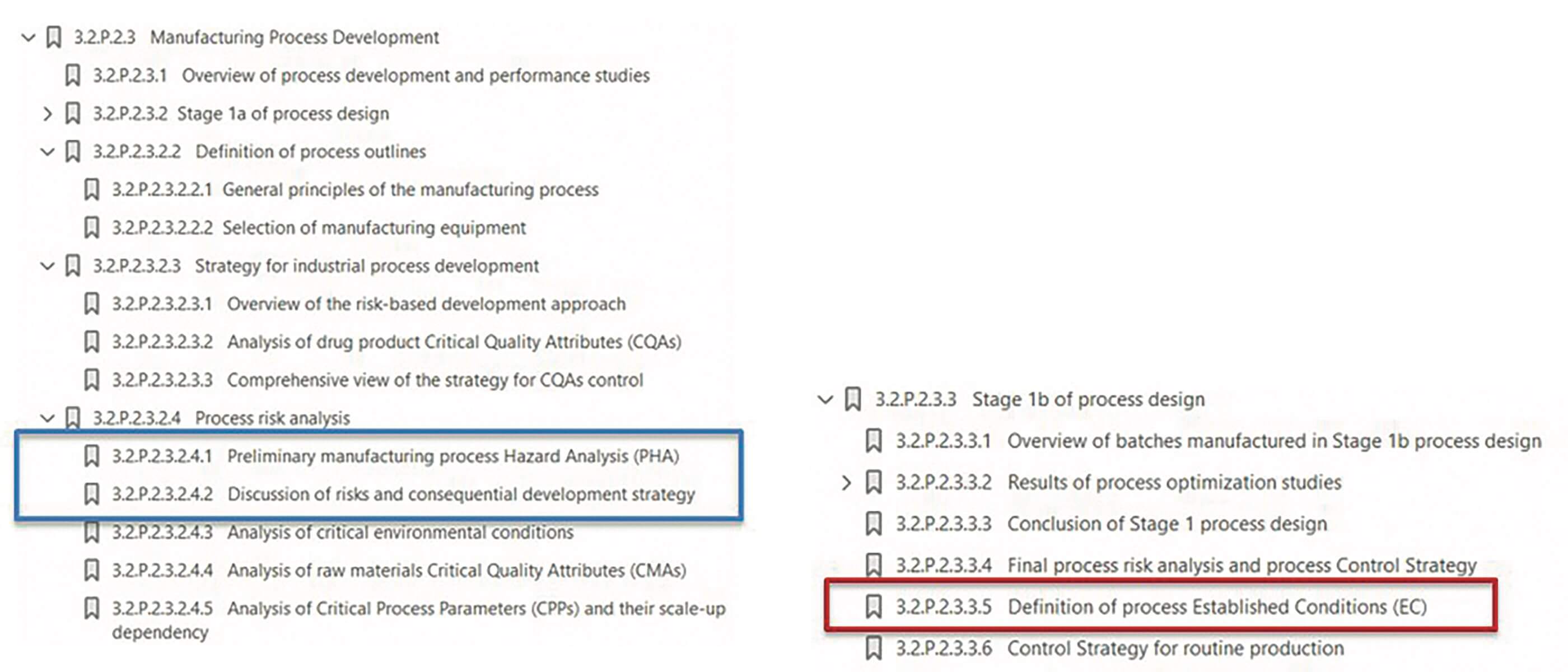
Based on the experience of three different dossiers submitted, we established a general template for the process development subsection as presented hereafter.
This work will probably be refined in a continuous improvement spirit, but is currently the starting point of our new dossiers written in CTD.
The main options chosen for writing pharmaceutical development sections were to:
• Present the QTPP in introduction and the analysis of CQAs right after the discussion on the choice of the manufacturing process outlines.
• Present the proposed routine Control Strategy (control points) as a conclusion of the final process risk assessment. Detailed description of control points being described in the relevant sections describing routine manufacturing and control operations.
• Present a stepwise approach of process development, with: process design, initial risk assessment (PHA), process optimization and scale-up strategy, development results and conclusion on the proposed Control Strategy, identification of ECs and ECs classification
• Anticipate a subsection to allow for post-approval supplementation when additional product knowledge is gained (potentially leading to adjustments to the Control Strategy)
It was also decided to better value the Quality Overall Summary(10) (11) to make it a key document presenting the approach taken in the dossier (with location of data), a summary of QbD elements and proposed ECs.
Regarding process development, two main phases are presented in the dossier:
• Choice of the manufacturing process, generally performed based on laboratory and pilot trials (=Stage 1a of process design).
• Process understanding and optimization of the process, based on a risk assessment progressively refined throughout development (=Stage 1b of process design)
The underlying rationale supporting the definition of ECs mainly derive from this second phase of step 1b in which process risk assessment plays a key role.
Process risk analysis is a common practice for development and production departments. However, as for any risk analysis, it should be presented considering the objective of the exercise.
The initial process risk analysis presented in CMC dossiers in introduction to process development studies aims at giving an overview of the risk area specific to the drug product and at justifying the process development plan. The risk assessment methodology used in the CMC dossier was therefore defined to this end.
8. Initial Process Hazard Analysis (PHA) to support identification of risk area
Among the risk management tools listed in section 5 of ICH Q9, two were applied to structure development data in the CMC dossier: Process Hazard Analysis (PHA) and risk ranking.
Examples of Process Hazard Analysis used to support pharmaceutical development can be found in the literature as well as in regulatory documents posted on Authorities websites (12)(13)(14). Process risk area are generally presented using three qualitative risk levels, indicated by three different colors, which gives a concise summary view.
The principle is to only consider severity and probability of occurrence. Indeed, before optimizing the process, detectability should not be considered to rank quality risks, the objective of process development being to first mitigate all process risks. Only when this is done, can detectability be introduced to justify the routine Control Strategy reducing remaining risks to acceptable levels(15).
However, how to assign the three level of risks is not addressed, which was not found satisfactory for the regulatory dossier.
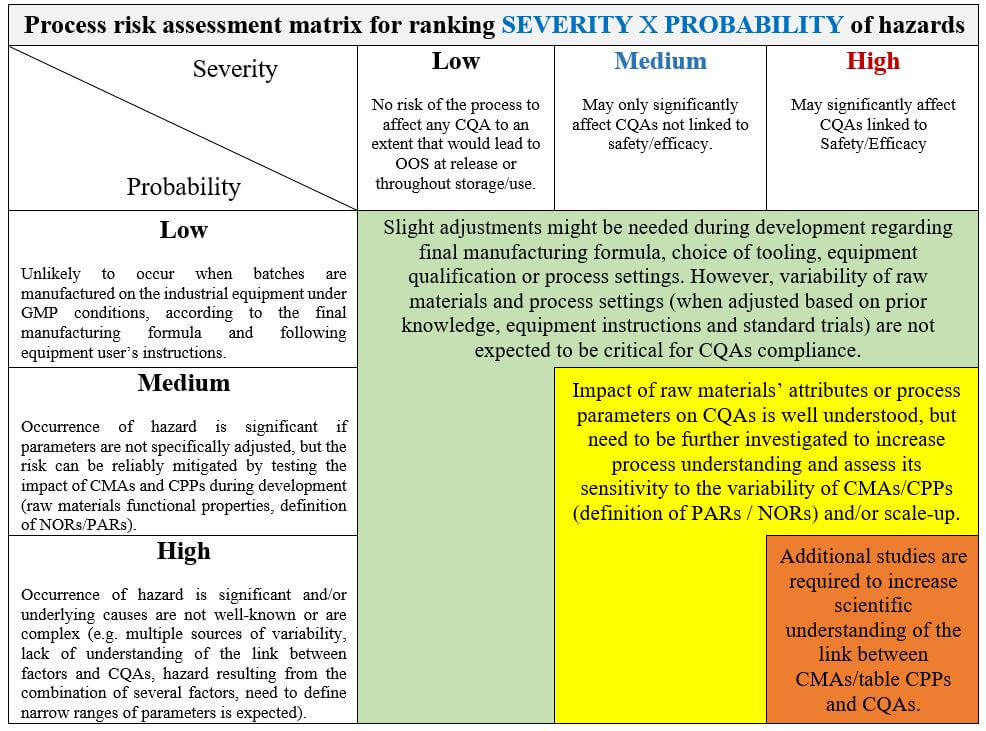
A specific matrix was therefore established to present clear and objective criteria for ranking process risks. For the severity of risks, the criteria considered was the type and extent of impact on CQAs. For the probability of risks, the criteria was the extent and complexity of development studies needed to reduce probability of occurrence (e.g. no specific studies required for risks being controlled through GMPs, or need to further investigate process conditions).
The risk matrix used is presented in figure 3.
It is important to stress here that presenting a cross-analysis Unit operation x CQAs and just attach the risk matrix is not enough to support the risk assessment. Risk ranking should be explained with a science-based discussion of the potential impact of the process on product CQAs. A useful example can be found in 2012 FDA example(14) “Quality by Design for ANDAs: Immediate-Release dosage forms QbD IR tablet Module 3 Quality” (pages 52-54).
Eventually, the option selected for our dossiers was to present two key summary tables supporting the process risk assessment:
• A cross-analysis table Unit operations x CQAs (in which a short description of each risk was added to have a more complete table)
• A tabulated summary of risk ranking justifications (in which we also added a short summary of development studies performed to characterize the process and mitigate risks, including scale-up considerations)
More detailed explanations are presented in subsequent process development sections, but tabulated summaries can be used as a convenient entry point to the development rationale presented in the dossier.
In the following subsections, process development results are discussed in more or less details according to the level of risks and the complexity of studies. The idea is here not to detail unit operations covered by GMPs (or for which no specific adjustment/tight control is required), but focus on the specific risk area of the drug product and knowledge gained during development.
Further analysis of CPPS being required, other risk analysis tools may be useful (e.g. Ishikawa diagram). For processes considered in this pilot phase, CPPs were quite obvious without requiring any additional formal risk analysis for their identification.
However, being at the same time focused on risk area but comprehensive in the process risk analysis was not always easy, and each dossier may raise different challenges with this regard.
9. Classification of process parameters to assign ECs reporting categories
In regulatory guidelines, parameters are typically referred to as critical or non-critical. However, this is rarely that binary in real life, even for non-biotechnological processes. We found it necessary to define several risk-based categories using a well-defined methodology consistent for all dossiers and transparent for reviewers.
First step: Identify ECs
Established Conditions (ECs) are defined by ICH Q12 as legally binding information considered necessary to assure product quality and requiring regulatory submission to Authorities in case of change.
However, identification of process risk area does not automatically results in ECs identification, and defining the exact nature of the critical process condition(s) sometimes need further analysis. Indeed, for some unit operations, Established Conditions may not be parameters but an input attribute (e.g. CMA) or a desired output attribute. In the latter case, parameters are adjusted to reach an “end of operation” target and may require readjustment during the product life cycle, e.g. to adjust to raw materials properties or following changes to the equipment. Two examples are described hereafter, in which process parameters were ultimately not defined as ECs of the unit operation:
An example of easy-to-adjust parameters: – mixing parameters for pharmaceutical solutions.
One example of an issue faced during dossier preparation for standard low risk pharmaceutical solutions was the classification of mixing parameters. Indeed, mixing speed and time generally only aim for efficient and complete dissolution before moving to the next addition step. For that purpose, mixing speed and time should be well defined in the routine instructions for operators. However, changes to these parameters are generally easy to do through a simple verification protocol without any risk to the product CQAs.
For this type of parameter, common sense tells us that it wouldn’t be relevant to submit a variation in Europe every time mixing parameters of the solution are adjusted/optimized (even not as a Type IAN). However, strictly applying the decision tree of ICH Q12 would qualify such parameters as ECs with minor impact, still requiring notification.
On the other hand, how could we present the EC as the end-point “until dissolution” when there is no routine IPC to check dissolution after each material addition. In other words, can we declare an “End-point” EC when the end-point control would be applied in case of changes but that it is not described in the routine manufacturing process in section 3.2.P.3?
This is what I call the “grey zone” of ICH Q12 guideline: it is obvious that changing some parameters are so easy that it can be reasonably managed under the PQS, but ICH Q12 guideline (as well as current EU regulation on variations) does not clearly cover such cases. In my opinion, this issue comes from the fact that there is confusion between two types of criticality assessment: from a quality management viewpoint (answering the question: what is the appropriate level of monitoring of the parameter on commercial batches?) or from a regulatory management viewpoint (answering the question: what is the appropriate level of regulatory supervision when the parameter is changed?). These two dimensions of parameters criticality can combine differently, which is not reflected in Figure 1 of ICH Q12.
In the end, common sense led us to ask for not having changes to such mixing parameters managed under regulatory supervision for our EU dossiers (parameters classified as non-ECs), considering raw materials solubility properties, easy on-line control for full dissolution and detectability of failure on the finished product by routine release testing.
This approach is in line with the principles set by PACMPs, i.e. reduce the need for regulatory supervision when providing the description of how changes will be done under the applicant’s PQS. This led to downgrading changes of these minor risk CPPs from regulatory notification to management under the applicant’s PQS.
Two concrete examples of how this approach was taken in our dossiers are provided hereafter:
• For one dossier submitted in Europe, in the step at which API is added, the API is freely soluble but is sensitive to acidic pH conditions. The mixing speed was not declared as an EC. ECs were identified as: a short 15 minutes minimum mixing time, and the maximum time the API is left in acidic solution before moving to the next step (at which the pH increases).
• In another European dossier, for the API addition step, it was particularly important to ensure efficient incorporation/dispersion of the powder due to the dissolution rate and also the absolute need to obtain full dissolution before the next step. The mixing speed was not declared as an EC. ECs declared for this addition step were: adjustment of mixing parameters to create a vortex on the surface, minimum mixing time of 90 minutes and product temperature.
As can be seen from these examples, parameters classification and identification of ECs were justified considering the raw materials properties and the process risk area specific to each product.
• An example of on-line adjustment: target filling volume of liquid forms
A second example is the control of the filling operation to ensure that the volume delivered by all containers is between the minimum and maximum acceptable limits (limits justified considering container specifications, product physicochemical properties and dose label claim). What is important here is to ensure that extractable volumes comply with label claims and pharmacopoeia standards: accuracy of doses for single dose products, number of doses or minimum volume for multidose products.
However, the acceptance limits of the filling volume IPC should also consider the performances of the filling line, whose capability may change with time or following changes to the equipment.
For one multidose liquid product, the acceptable limits for the extractable volume were first justified in the dossier considering container specifications and label nominal volume, but no fixed limits were defined for the filling volume IPC. Instead of setting fixed IPC limits, the EC declared for this in-process control point was the calculation procedure of the on-line lower and upper control limits (bottles weight control). The calculation formula was detailed and is based on the brimful volume of bottles, the volume occupied by the closure system, the remaining volume in emptied bottles and the capability of the filling line). By focusing on the actual CQA impacted (extractable volume), this allows for post-approval adjustment of the target filling volume to equipment performances, hence both ensuring better control of CQAs and optimization of production costs.
These two examples pertain to simple low risk unit operations, but they quite well illustrate the type of debate triggered by this first step of ECs identification.
Second step: Assign reporting categories to ECs
For assigning risk categories to process parameters, it should be possible to establish general risk ranking criteria, independently from the product specific risk area. But regulatory guidance is vague in this regard.
We can note that the link between risk levels and reporting categories are well described in Figure 1 of ICH Q12, but that the methodology for ranking risks is not addressed. Simple reference to ICH Q9 is not helpful when it comes to concretely classify parameters, which may lead to very different interpretations and give a lot of uncertainty as to the acceptability of the proposed strategy for ECs changes. With the objective to secure this point, we chose to clearly present the logic for ECs classification in the dossier. Some ideas came from articles found in the literature dealing with parameters criticality analysis for non-biological products (16) (17).
Several criteria seemed important when proposing ECs reporting categories:
• Understanding of CQAs sources of variability
• Interaction between parameters (can parameters be assessed separately? do parameters only impact the output of the unit operation to which it applies?)
• Easiness of adjustment
• Ability of the control strategy to detect failure (direct observation, on-line measurement, at release or in stability)
In one of our dossier, we presented our classification rules in a summary table to support the proposed strategy for post-approval change management. The classification led to several categories, with for instance some parameters classified as “well-controlled parameters” because not requiring tight specific control, and whose adjustment can easily be done through simple on-line verification. These type of parameters typically lies in what I called previously the “grey zone” of ICH Q12, that is, parameters to specify in Master Batch Records for operators, but not requiring regulatory oversight. These changes can be easily managed under the PQS through a simple plan, without any need for a formal protocol.
In our first dossier submitted in USA, such parameters were declared as ECs whose change would be notified in the annual report (through communication of the updated Master Batch Record). In the two next dossiers submitted in Europe, these parameters were presented as non-ECs (change management documentation kept on site, as no annual report exists that would allow us to report it easily).
Regarding this “grey zone” concern, we chose to adopt a pragmatic approach, assuming that provided appropriately justified, Authorities would also be pragmatic and consider the initial objective of the guideline, that is, adjust the level of regulatory oversight to the level of risk and reduce the number of regulatory variations.
Even if an internal tool for risk ranking of process parameters can be defined by companies, some guidance on the methodology to assign risk levels to process parameters (decision matrix, decision trees, examples for different pharmaceutical forms) would be welcome to complete ICHQ12, for better understanding of Authorities expectations and for harmonization purposes across regions.
Concrete examples and agencies feedbacks
Three case-studies are discussed hereafter. At present we received the first list of questions for all dossiers:
For case 1 (US FDA procedure), the need to have both a comprehensive analysis of ECs and a clear concise overview proved to be a first challenge. The will to be exhaustive turned into confusion for reviewers. Moreover, no link with current applicable guideline for variations being presented, this may have given the impression that current guidelines were circumvented. The answer is under preparation, with additional analysis against CVM guideline #83 on variations and a summary table presenting ECs, non-ECs and justifications.
For case 2 (EU centralized procedure), due to time constraints for the preparation of the dossier, justifications of ECs were incomplete and tabulated comprehensive summaries were lacking. For one unit operation, the justification of the proposed limits for ECs was not sufficiently supported. PARs, NORs and the routine process operating space required further scientific justifications. The answer was just sent, with further justification and a summary table clearly presenting ECs, non-ECs and justifications. Updated dossier sections were also prepared (pharmaceutical development section completed with additional data analysis, revised process section clearly identifying ECs in the process description).
For case 3 (EU centralized procedure), the dossier was built on an important amount of development but also production data (product existing on some markets for several years), leading to a retrospective QbD approach. This was the last dossier submitted with ECs and it benefited from the experience of the preparation of the two other dossiers. We didn’t get any questions on ECs.
Lessons learned from these three pilot dossiers already allowed us to identify some rules to be applied for next dossiers:
• Pharmaceutical development section: provide a clear summary table of ECs, also including non-ECs, along with short justifications
• Process section: clearly distinguish in the description of the process ECs from non-ECs, as well as distinguish routine NORs from parameters ranges as defined by EMA Q&A guidance (EMA/CHMP/CVMP/ QWP/354895/2017). Different fonts and/or brackets can be used in the same sprit as what is done in Japanese CMC dossiers, which is also helpful for production and quality departments.
• Quality Overall Summary: highlight consistency with current regional guidelines dealing with reporting categories of regulatory variations
This pilot phase having only dealt with liquid solutions, we are aware that additional questions will probably arise when dealing with more complex manufacturing processes (e.g. solid dosage forms), requiring further adjustments to our methodology and its presentation in CMC dossiers.
Conclusion
From a company’s perspective, the first obvious advantage of adopting ICH Q12 is to distinguish ECs from other elements provided for information in CMC dossiers. Our first steps towards ICH Q12 consisted in experimenting the acceptance of the concept of ECs from European and US regulatory veterinary Agencies with the submission of several pilot dossiers.
But one cannot jump directly to the declaration of ECs without some preparation. In our case, the first prerequisite was to reinforce the scientific basis of our CMC dossiers to increase the movement from mainly descriptive dossiers toward science-based dossiers highlighting the risk area specific to each drug product. This was done by introducing QbD concepts in CMC dossiers.
In the absence of any relevant ICH or regional guidance, it was also deemed important to establish a suitable structure of pharmaceutical development subsections and to define an internal methodology for regulatory oriented process risk analysis and for risk-based classification of process parameters. With this revised structure and role, the pharmaceutical development section becomes central in the CMC dossier. The QOS also becomes a key element for presenting to regulatory reviewers the approach taken for each dossier.
One other challenge was to present comprehensive justifications in a clear and concise way. It also proved to be a key success factor for getting approval from Authorities, most of the questions received originating from either lack of data analysis or lack of clear summaries for an easy review of the proposed strategy.
As a conclusion, we can say that our first experience of ECs submission in dossiers resulted in a positive outcome. It appeared that EU and US Authorities were open to ECs even though ICH Q12 was not yet approved, provided appropriately justified and consistent with local regulation. For the latter point, this reminds us that, even if regional EU and US regulation already contains provisions compatible with the concept of ECs, it should be carefully assessed how far the approach can be taken not to conflict with regional requirements. We should therefore keep on watching the evolution of each regional Health Authority’s policy in the coming years. Upon ICH Q12 approval, a transitional period is indeed foreseen for fully integrating the new concepts in regional guidelines but also in review practices.
One other important aspect not discussed in this article is the changes this new approach is bringing to organizations and working processes, with a need for increased collaboration between development and production teams and early involvement of CMC dossier writers.
Partager l’article


Viviane Neron De Surgy – VETOQUINOL
Responsable de la rédaction des dossiers CMC des nouveaux produits vétérinaires et de la veille réglementaire CMC chez Vetoquinol et vice-chair du groupe Qualité de Animalhealth Europe. De formation ingénieur agronome avec une spécialisation en chimie analytique, Viviane a exercé différents postes en Production, Qualité et Compliance réglementaire avant de se spécialiser dans le domaine de la CMC réglementaire dans l’industrie humaine puis vétérinaire.
Bibliography
Current regulatory texts:
(1) EMA guideline EMA/CHMP/QWP/245074/2015 “Manufacture of the finished dosage form”, 2017
(2) EMA/CHMP/QWP/104223/2016 “Overview of comments received on ‘Draft Guideline on manufacture of the finished dosage form’ ”, published in July 2017 (see page 2 comments on the level of detail to include in regulatory dossiers)
(3) EMA draft guideline EMA/CVMP/QWP/798401/2015 “Guideline on Manufacture of the Veterinary Finished Dosage Form”, 2018
(4) Guidelines on the details of the various categories of variations, on the operation of the procedures laid down in Chapters II, IIa, III and IV of Commission Regulation (EC) No 1234/2008 of 24 November 2008 concerning the examination of variations to the terms of marketing authorisations for medicinal products for human use and veterinary medicinal products and on the documentation to be submitted pursuant to those procedures.
(5) FDA CVM guidance “CVM GFI #83 Chemistry, Manufacturing and Controls Changes to Approved NADA/ANADA”, May 2007
(6) FDA CDER guidance “Changes to an Approved NDA or ANDA”, 2004
(7) FDA CDER guidance for industry “Changes to an Approved NDA or ANDA: Questions and Answers”, January 2001
(8) Draft FDA CDER guidance “Established Conditions: Reportable CMC Changes for Approved Drug and Biologic Products”, 2015
(9) FDA CVM guidance #234 “Question-Based review for the Chemistry, Manufacturing, and Controls technical section of animal drug applications”, 2016
Role of the Quality Overall Summary:
(10) “A Regulatory Perspective on the Quality Overall Summary: Putting the Pieces Together”, FDA Office of Pharmaceutical Quality (OPQ), 2018
(11) “Quality Overall Summary Grounds for Revision”, Jean-Louis Robert, 2006
Presentation of QbD approach and process risk analysis in dossiers:
(12) Pharmaceutical Development Case Study: “ACE Tablets” prepared by the Conformia workshop (CMC‐IM Working Group), March 13, 2008
(13) Common technical document [CTD] section 3.2.P.2 called ‘Mock P.2 for “Examplain” Hydrochloride’, prepared in 2006 by the European Federation of Pharmaceutical Industries Association (EFPIA)
(14) Example of pharmaceutical development report “Quality by Design for ANDAs: An Example for Immediate-Release Dosage Forms”, FDA, April 2012
(15) “Considerations Regarding the Use of Detectability In Risk Assessments” by McFarland, Amanda Bishop, Waldron, Kelly (Journal of Validation Technology, Dec. 2015, Vol. 21 Issue 4)
(16) “PQLI Key Topics – Criticality, Design Space and Control Strategy”, Thomas Garcia, Graham Cook and Roger Nosal (J Pharm Innov (2008) 3:60–68, DOI 10.1007/s12247-008-9032-4)
(17) “Using a Systematic Approach to Select Critical Process Parameters”, Thomas A. Little, PhD (Pharmaceutical Technology Volume 2012 supplement, Issue 6, Nov. 2012)
Glossary
API: Active Pharmaceutical Ingredient
CMA: Critical Material Attribute
CMC: Chemistry, Manufacturing and Controls
CPP: Critical Process Parameter
CQA: Critical Product Attribute
CS: Control Strategy
CTD: Common Technical Document
CVM: Center for Veterinary Medicine (FDA division)
EC: Established Condition
GFI: Guidance For Industry (FDA)
GMP: Good Manufacturing Practices
ICH: International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use
IPC: In-Process Control
PACMP: Post-Approval Change Management Protocol
PHA: Process Hazard Assessment
PQS: Pharmaceutical Quality System
Q&A: Questions and Answers
QbD: Quality by design
QOS: Quality Overall Summary
QTPP: Quality Target Product Profile
VICH: International Cooperation on Harmonisation of Technical Requirements for Registration of Veterinary Medicinal Products
